If you’ve never had heartburn before and suddenly it’s showing up every day in your 40s, you’re not alone. Perimenopause GERD is one of the most common, yet least talked about digestive issues midlife women deal with, and most of them have no idea their hormones are behind it.
If you’re waking up at 2am with burning in your chest, reaching for antacids before meals just as a precaution, or you’ve tried cutting out coffee and wine and spicy food and still not getting relief — this post is for you. No one has connected any of this to perimenopause and what’s happening to your body. But there’s a lot more going on than you’ve been told.
Research shows that a staggering 42% of perimenopausal women report upper GI symptoms including heartburn and reflux — with 80% of them never receiving a formal diagnosis (1).
The standard response is a prescription for a proton pump inhibitor (a medication that reduces stomach acid production). Sometimes that helps. But it does nothing about the hormonal, gut motility, microbiome, and lifestyle drivers that caused the problem in the first place.
I’m Sarah Neumann Haske, MS, RDN — a gut health dietitian with over 20 years of clinical experience, specializing in perimenopause and digestive health for the past 10 years. In this post I’ll walk you through why perimenopause GERD happens, what’s actually driving it, and what a root-cause approach looks like. GERD is just one piece of a bigger gut picture, learn more about working with a Perimenopause Gut Health Dietitian.
Want to start understanding your gut symptoms better right now?
- Download the free 5-Day Gut Healing Plan — five days of what I teach my clients from day one.
- Or book a free Digestive Assessment Call to see if my 3 month gut coaching program is the right fit for you.
- If you’re struggling with IBS symptoms on top of GERD, my Midlife IBS Quiz takes 3 minutes to assess whether hormones are playing a role.
What Is Perimenopause GERD?
Before we get into the root causes it’s worth getting clear on terminology because these terms get used interchangeably and they don’t all mean the same thing.
- Acid reflux is the physical event — stomach acid traveling back up into the esophagus. It can happen occasionally in anyone and doesn’t automatically mean something is wrong.
- Heartburn is the symptom — that burning sensation in the chest or throat that happens when acid irritates the esophageal lining. You can have heartburn without having GERD.
- GERD (gastroesophageal reflux disease) is the diagnosis — defined clinically as acid reflux occurring at least twice a week, causing bothersome symptoms, or producing measurable damage to the esophagus. It’s a chronic condition, not just occasional discomfort.
- Perimenopause GERD specifically refers to GERD that develops or significantly worsens during the hormonal transition of perimenopause — driven by the same underlying changes in hormones, gut motility, microbiome, and gut lining integrity that we cover throughout this post.
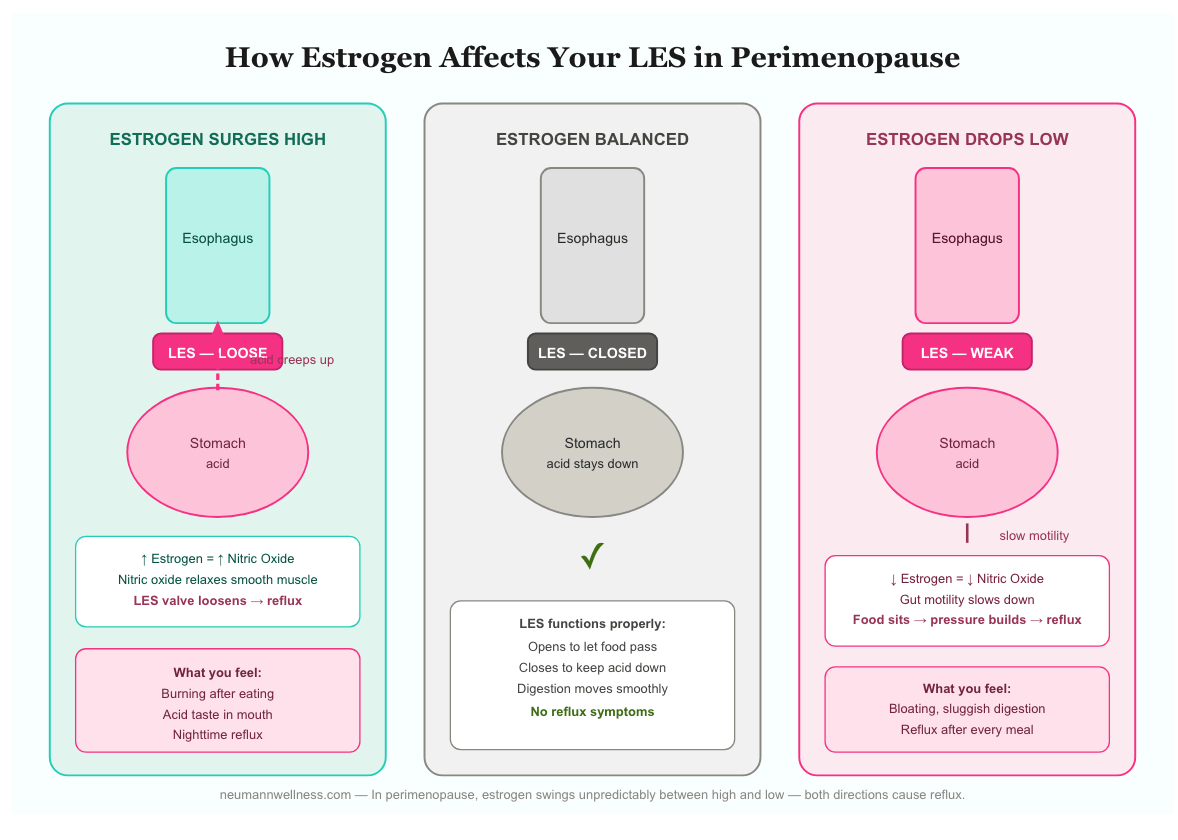
Between your esophagus and your stomach sits a muscular valve called the Lower Esophageal Sphincter (LES). It acts like a one-way door — opening to let food pass into your stomach then closing tightly to keep everything in. When that door doesn’t close properly stomach acid travels back up. The esophagus doesn’t have the same protective lining as the stomach so acid causes that burning sensation most people recognize as heartburn.
Perimenopause GERD symptoms include:
- Burning in the chest or throat, especially after eating or lying down
- A sour or bitter taste in your mouth
- Waking at night with burning or coughing
- A sensation of food or liquid coming back up
- Difficulty swallowing or a feeling of something stuck in your throat
- Chronic hoarseness or a persistent cough with no clear cause
- Worsening symptoms after coffee, alcohol, acidic foods, fatty meals, or lying down after eating
If these symptoms have gotten significantly worse since perimenopause started, the hormonal connection is worth understanding.
Why Perimenopause GERD Happens — The Hormone Connection
Perimenopause starts when estrogen and progesterone begin to fluctuate and eventually decline. These wide fluctuations in hormones typically begins in your early to mid-40s and progressively decline from there. This hormonal shift can affect your entire digestive system, so sometimes you might notice lower gastrointestinal issues (like constipation, bloating, diarrhea) along with reflux. Perimenopause GERD develops because of several interconnected changes happening simultaneously.
Estrogen’s Role in Perimenopause GERD
Estrogen does a lot more than regulate your cycle. It’s actively involved in how your digestive tract functions, and when it starts behaving unpredictably in perimenopause, your esophagus feels it. Here’s why.
Why Estrogen Fluctuations Make Perimenopause GERD So Unpredictable
What makes perimenopause particularly disruptive is that estrogen doesn’t follow a predictable path. Research shows that estrogen levels fluctuate significantly during perimenopause and those patterns differ considerably from woman to woman (2). There’s no neat decline your body can gradually adapt to.
Instead, estrogen can swing high and then crash low within a short window of time, and your gut is reacting to every single shift. That unpredictability is a big part of why perimenopause GERD feels so random and so hard to pin down to a specific food or trigger.
How Estrogen Affects Nitric Oxide Production
Estrogen increases the production of nitric oxide in the body. Most people have heard of nitric oxide in the context of heart health or athletic performance, but it’s actually a signaling molecule your body produces naturally and uses everywhere. Its main job is to relax smooth muscle. It widens blood vessels to improve circulation, helps regulate blood pressure, and keeps the muscular valves and tubes throughout your digestive tract functioning properly.
Your body makes nitric oxide two ways. The first is directly from an amino acid called L-arginine, a process that requires micronutrients like vitamin B2, folate, vitamin C, magnesium, and zinc to work properly. This is exactly one of the many reasons why I include micronutrient testing in my 3 month Perimenopause gut healing program.
The second is from dietary nitrates found in foods like leafy greens, beets, and celery. When you eat those foods, your oral and gut bacteria convert the nitrates to nitrites, and then your stomach converts that nitrite into Nitric Oxide (NO) (3).
What Nitric Oxide Does to Your Esophageal Valve
In the context of your esophagus, nitric oxide relaxes the Lower Esophageal Sphincter (LES). The LES is the valve between your esophagus and stomach that keeps food and acid where it belongs. When this valve is working properly, it opens to let food down and closes tightly to keep acid from creeping back up.
Nitric oxide is part of what regulates the LES opening and closing.
When estrogen rises, nitric oxide production rises with it, the LES valve loosens, so acid and food has an easier time traveling up your esophagus, in the wrong direction (4).
At the same time, when estrogen drops, nitric oxide production drops with it too, and while that might sound like it would help reflux, the gut lining and the muscles that keep digestion moving also depend on proper nitric oxide signaling (5, 6).
Therefore estrogen swinging too high or too low both disrupt the LES functioning.
How MRT Food Sensitivity Testing Connects to Perimenopause GERD
Mediator Release Testing is a food sensitivity test that looks at your reactivity to both nitrates and nitrites as separate food chemicals. These are two different things.
If your MRT results show reactivity to nitrates or nitrites, removing them is absolutely the right first step to calm your immune system and give your gut a chance to repair. But that reactivity is also telling us something deeper is going on.
A healthy and diverse oral microbiome is essential to converting dietary nitrates into nitric oxide properly (7). If your oral microbiome is off — from using antiseptic or antiplaque mouth rinses, gingivitis, or periodontal disease — that conversion gets compromised and nitric oxide production suffers as a result (8)
The reactivity on your MRT is often a sign of that underlying microbial disruption, not a permanent problem with the foods themselves. It’s exactly why combining food sensitivity testing along with comprehensive stool testing is such an important part of getting to the root of what’s driving your GERD symptoms.
Estrogen HRT and Perimenopause GERD
If you’re in perimenopause also adding estrogen through HRT, that’s a separate layer that can amplify the effect on your LES. A large study of over 51,000 postmenopausal women found that current estrogen-only HRT users had a 66% increased risk of GERD symptoms, with risk climbing higher with both increasing dose and duration of use (7). The mechanism is the same in perimenopause. If your reflux got worse after starting HRT, this is likely a piece of why.
Progesterone and Perimenopause GERD
Progesterone acts as a smooth muscle relaxant throughout the body, and that includes the LES (8).
Research confirms that higher progesterone levels reduce LES pressure, which helps explain why heartburn is so common in pregnancy or with HRT — high progesterone keeps that valve loose (9).
In a normal menstrual cycle, reflux symptoms tend to be more common in the luteal phase (the second half of your cycle, after ovulation), when progesterone is at its highest (10). That’s the progesterone-LES connection playing out month to month.
In perimenopause, progesterone doesn’t simply drop in a straight line. Research shows it fluctuates significantly and unpredictably, and those patterns differ from woman to woman throughout this phase of their life (2). So the effect on your LES isn’t as simple as “less progesterone means less reflux.” The instability itself is part of the problem.
It’s also worth noting that low progesterone in perimenopause might theoretically help reflux by reducing that relaxing effect on the LES. But research suggests that doesn’t seem to outweigh the much stronger connection between low estrogen and GERD (11). Estrogen appears to be the more dominant hormonal driver, which is why we covered it separately in the above section.
Progesterone HRT and Perimenopause GERD
If you’re on HRT, this is worth paying attention to. Progesterone is added to HRT for two reasons. For women who still have a uterus, estrogen taken alone causes the uterine lining to thicken over time, raising the risk of uterine cancer.
Progesterone is added to counteract that effect. It also helps with perimenopause symptoms like poor sleep, hot flashes, night sweats, and mood changes. But because progesterone is a smooth muscle relaxant, adding it back through HRT can loosen the LES enough to let acid creep back up (12).
Some research does suggest that women taking HRT during perimenopause and menopause experience more reflux (13). That said, most of this research has looked at synthetic hormone formulations.
We don’t yet have strong data on whether bioidentical hormone replacement therapy (BHRT) — the safer, more individualized option increasingly used in practice today — carries the same risk.
If your reflux started or got noticeably worse after starting HRT, the progesterone component is likely part of the picture. That doesn’t mean HRT is wrong for you. It just means your reflux deserves to be part of the conversation with whoever prescribed it.
Gut motility slows down
As discussed earlier, estrogen and progesterone regulate the smooth muscle contractions that move food through your digestive system. When these hormones fluctuate in perimenopause, gut motility slows down (14). When things slow down in your digestive tract, food sits in your stomach longer, pressure builds, and acid has more opportunity to creep back up.
Bloating increases pressure on the LES
Bloating is one of the most common perimenopause symptoms — and it directly worsens perimenopause GERD. When your abdomen is distended from gas or slowed digestion, the pressure inside your abdominal cavity increases. That pressure pushes upward against the stomach and the LES. Even a well-functioning LES can be overwhelmed by enough upward pressure (15).
This is also where the overlap between perimenopause GERD and IBS becomes clinically important. Many perimenopausal women are dealing with both at the same time without realizing it.
The bloating, gas, and altered gut motility that drive IBS symptoms are the same mechanisms feeding the reflux. If you’re treating your GERD without addressing the underlying gut dysfunction driving your bloating, you’re only managing half of the picture.
Research confirms that bloating and distension commonly coincide with other functional gastrointestinal disorders including IBS and functional dyspepsia (16). In perimenopause, when hormonal changes are disrupting both gut motility and the gut microbiome simultaneously, these conditions very often show up together.
The microbiome shift contributes
Estrogen decline can also disrupt the gut microbiome — reducing beneficial bacteria and allowing less favorable populations to grow (17). A disrupted gut microbiome drives gas production, bloating, and slowed motility — all of which worsen perimenopause GERD. It also drives low-grade gut inflammation that makes the esophagus more sensitive to acid.
Read more about how the microbiome connects to hormone health here.
Stress and cortisol amplify everything
Perimenopause is physiologically stressful. Cortisol slows digestion, increases gut permeability, and alters nervous system regulation of the digestive tract (18). High cortisol also increases stomach acid production (19). When the LES is already compromised and gut motility is already slow, elevated cortisol pushes perimenopause GERD symptoms further.
Read more about the mind-gut connection and how stress drives digestive symptoms here.
Other Factors That Drive Perimenopause GERD
Hormones get most of the attention when it comes to perimenopause GERD — and for good reason. But for many women, there are structural, lifestyle, and physiological factors driving their reflux that have nothing to do with hormones and everything to do with what’s happening in their body day to day.
Hiatal hernia
A hiatal hernia happens when part of the stomach pushes up through the diaphragm — the muscle separating your chest from your abdomen. This structural change positions the LES higher than it should be, making it far easier for acid to travel upward. Hiatal hernias are more common in women over 40 and frequently go undiagnosed. Many women with perimenopause GERD that doesn’t respond to dietary changes have an undetected hiatal hernia contributing to their symptoms. An upper endoscopy identifies one reliably.
What Actually Causes a Hiatal Hernia
From a conventional standpoint hiatal hernias are often attributed to age, obesity, or just bad luck. From a functional medicine perspective the picture is more nuanced. The diaphragm and surrounding connective tissue need adequate tone and structural integrity to keep the stomach where it belongs. When that integrity is compromised, the stomach can gradually migrate upward. Common contributors include (20):
- Chronic constipation and straining — years of bearing down during bowel movements significantly increases intra-abdominal pressure and is one of the most underrecognized drivers. This is one more reason perimenopause and menopause constipation isn’t just uncomfortable — it has downstream structural consequences.
- Chronic coughing — from allergies, asthma, or postnasal drip, repeated forceful coughing increases thoracic and abdominal pressure over time.
- Heavy lifting without proper breathing mechanics — breath-holding during exertion repeatedly spikes intra-abdominal pressure.
- Connective tissue hypermobility — women with hypermobile Ehlers-Danlos syndrome (hEDS) or generalized joint hypermobility have inherently lax connective tissue throughout the body, including the ligaments and fascial structures that anchor the stomach and diaphragm. If you’ve been told you’re hypermobile or have received an hEDS diagnosis, this connection is worth exploring with a knowledgeable practitioner.
- Chronic stress and diaphragmatic tension — a chronically activated stress response causes the diaphragm and surrounding muscles to hold tension in ways that alter pressure dynamics around the gastroesophageal junction over time.
Visceral Manipulation
One of the most underutilized approaches for hiatal hernia is visceral manipulation — a hands-on manual therapy performed by specially trained physical therapists and massage therapists that works directly with the mobility and positioning of the internal organs and surrounding connective tissue.
For a hiatal hernia, a trained practitioner can work to gently release the stomach from its elevated position and restore normal diaphragmatic mobility. Many women report significant improvement in reflux symptoms after a series of sessions, often alongside dietary and lifestyle changes. To find a qualified practitioner, search the Barral Institute’s directory here: Find a Visceral Manipulation Practitioner.
Getting a Proper Diagnosis
If your perimenopause GERD hasn’t responded to dietary changes, ask your gastroenterologist specifically about hiatal hernia during an upper endoscopy. Small hiatal hernias are frequently noted but not discussed with patients — and they may be more relevant to your symptoms than anyone has told you.
Medications that worsen perimenopause GERD
Several medications commonly used in midlife worsen perimenopause GERD by relaxing the LES, increasing acid production, or irritating the esophageal lining directly:
- HRT: Both estrogen and progesterone-containing HRT have been associated with increased GERD risk (21). If your reflux worsened after starting HRT, that connection is worth discussing with your prescribing doctor or finding a provider who prescribes BHRT (Bio-identical hormone replacement therapy) as we discussed above may be better tolerated for GERD.
- NSAIDs: Ibuprofen and naproxen irritate the stomach lining directly and weaken its protective mucus layer (22)
- Calcium channel blockers: Used for blood pressure, these relax smooth muscle including the LES (23)
- Benzodiazepines: Relax the LES and slow gastric emptying (24, 25)
- Certain antidepressants: Both tricyclics and some SSRIs affect esophageal motility and LES function (26, 27)
- Bisphosphonates: Used for bone density, these can cause esophageal irritation when not taken correctly (28)
Alcohol and coffee
Both alcohol and coffee relax the LES and increase stomach acid production. They’re among the most consistent perimenopause GERD triggers. With the LES already compromised by hormonal changes, even small amounts can tip symptoms over the threshold. During active symptom management, reducing both significantly is worth trying.
Eating late at night
Lying down within two to three hours of eating drives nighttime perimenopause GERD reliably. Gravity helps keep stomach contents down when you’re upright. Remove that advantage with a full stomach and acid has a much easier path upward. This is one of the simplest and most effective adjustments available — and one clients most consistently resist until they actually try it. Try incorporating a walk after your evening meal to help support digestion.l
H. pylori infection
H. pylori is a bacterial infection that lives in the stomach lining. It disrupts normal acid regulation, damages the stomach lining, and alters gut motility in ways that contribute to reflux. H. pylori frequently goes undetected and untreated — and treating it when it’s present can dramatically improve perimenopause GERD that isn’t responding to other approaches. Read more about H. pylori and how it affects gut health here.
Food sensitivities
In perimenopause, new food sensitivities often develop as the gut lining becomes more permeable due to estrogen decline. These immune-mediated reactions drive chronic gut inflammation that worsens perimenopause GERD, bloating, and motility issues.
A randomized controlled trial found that GERD patients who were not responding to PPIs experienced a significant 50% reduction in symptoms after just one month on a diet based on individual food sensitivity testing (29).
This is exactly why identifying each woman’s specific reactive foods through proper testing gives a clearer and more targeted picture of what’s driving her inflammation — rather than putting everyone on the same blanket elimination diet.
Read more about food sensitivities here.
Nutrient depletions
Several nutrient deficiencies directly worsen perimenopause GERD. Magnesium supports smooth muscle function including the LES. Zinc carnosine supports the integrity of the stomach and esophageal lining (30). B vitamins support nerve function throughout the digestive tract (31).
Long-term PPI use depletes magnesium, B12, calcium, and iron — meaning women on PPIs for perimenopause GERD are frequently deepening their nutrient deficits over time (32, 33, 34, 35). Read more about the micronutrient testing I use in my practice here.
On top of that, the body uses up specific nutrients faster when it’s constantly trying to repair esophageal tissue from ongoing acid damage. Micronutrients to watch are vitamin A, vitamin C, zinc, glutamine, arginine, and more (36).
Why Your Stomach Acid Production Changes In Perimenopause
Stomach acid production in perimenopause is more nuanced than most people realize. Estrogen actually inhibits gastric acid secretion as estrogen receptors sit directly on the acid-producing cells in the stomach and suppress their activity.
Research shows women secrete approximately 40% less acid than men, partly due to estrogen’s suppressive effect. As estrogen swings from high to low in mid perimenopause and then steadily declines in late perimenopause, acid production shift as well — which helps explain why reflux worsens.
Stomach acid production is not only influenced by estrogen, but also by vagal nerve tone, micronutrients, and thyroid function. In perimenopause, these are all under pressure simultaneously.
- Estrogen receptors sit directly on the acid-producing cells in your stomach — as estrogen declines, those cells become more responsive.
- Vagal nerve tone, which triggers acid production the moment you see or smell food, weakens with stress, autonomic dysregulation, aging.
- Micronutrient deficiencies like including zinc, magnesium, and B vitamins, can affect gastric function and digestive enzyme activity
- Women with Hashimoto’s thyroiditis have a 10 to 40% chance of concurrent autoimmune gastritis that can directly affect stomach acid and digestion.
The result is a woman who gets prescribed a PPI and doesn’t address any of these underlying factors.
There’s an Autoimmune Connection Nobody Is Talking About
There’s a condition called autoimmune gastritis where the immune system attacks the stomach’s acid-producing cells directly. Its peak incidence in women is in their 40s and 60s. It’s three times more common in women than men. And it’s strongly associated with the autoimmune conditions that cluster in perimenopausal women — Hashimoto’s, rheumatoid arthritis, vitiligo, and type 1 diabetes.
The nutrient deficiencies it causes — low B12, iron, zinc, magnesium, and calcium — are the exact deficiencies perimenopausal women are told are hormonal or dietary. Many of them are neither. They’re the consequence of an immune attack on the stomach lining that nobody has tested for.
You can ask your doctor about anti-parietal cell antibodies and anti-intrinsic factor antibodies — these are markers most directly associated with autoimmune gastritis.
Celiac disease and gluten sensitivity
Celiac disease and non-celiac gluten sensitivity both alter gut motility, increase gut permeability, and cause esophageal symptoms including reflux (37). Both are worth ruling out — especially in women who also have bloating, fatigue, nutrient deficiencies, and brain fog alongside their perimenopause GERD.
Proper celiac screening starts with a tTG-IgA blood test plus total IgA — but only while you’re still eating gluten daily. If results indicate further investigation, the next step is an upper endoscopy with biopsy. For accurate results, gluten needs to be consumed daily for 4 to 6 weeks before the endoscopy. Here’s the caveat: going gluten-free before testing will invalidate your results (38).
The Medical Workup to Do Before Working With Me
Before diving into a functional nutrition approach to perimenopause GERD, get a proper medical evaluation. Some causes of reflux need medical management first. Here’s what to discuss with your doctor:
- Upper endoscopy: The most important investigation for persistent perimenopause GERD. It lets your doctor visualize the esophagus and stomach, identify a hiatal hernia, check for Barrett’s esophagus (changes in the esophageal lining from chronic acid exposure), ulcers in the stomach, rule out structural issues, and biopsy for Celiac disease.
- H. pylori testing: A breath test, stool antigen test, or biopsy during endoscopy. Simple and worth doing before spending months on dietary changes.
- Celiac disease panel: Tissue transglutaminase IgA, total serum IgA, anti-gliadin IgG, and HLA-DQ2/DQ8 genetic typing.
- Full thyroid panel: Hypothyroidism slows gastric emptying and worsens perimenopause GERD — and it’s frequently missed with TSH alone, get a full thyroid panel.
- Medication review: Go through every medication with your doctor and to identify anything potentially contributing to reflux.
Once more serious or structural causes are addressed, the functional nutrition approach can tackle the hormonal, microbiome, and dietary layers that conventional medicine doesn’t have the tools to fix.
Why a PPI Alone Won’t Resolve Perimenopause GERD
Proton pump inhibitors (PPIs) like omeprazole and pantoprazole do exactly what they’re designed to do — they reduce stomach acid production. While they reduce your symptoms, they don’t address why you have GERD in the first place.
As discussed earlier, stomach acid is essential for digesting protein, absorbing B12, magnesium, calcium, and iron, and protecting against gut infections. Long-term acid suppression impairs all of these functions.
For women in perimenopause this is particularly concerning because declining estrogen is already reducing bone density — and PPIs compound that risk by further impairing calcium and magnesium absorption. Research confirms that long-term PPI use is associated with a significantly increased risk of hip, wrist, and spine fractures (39).
This is a conversation worth having with your doctor if you’ve been on a PPI for more than a few months. Many women also find their symptoms return when they try to come off PPIs — because the underlying drivers were never addressed in the first place. Read more about what’s really driving acid reflux here.
What a Root-Cause Approach to Perimenopause GERD Looks Like
Because perimenopause GERD is multifactorial, the approach needs to address all contributing layers. Here’s how I work through it with clients.
Eat slowly and mindfully
Eating quickly means swallowing more air — which increases bloating and upward pressure on the LES. It also means larger food particles entering the stomach, requiring more acid to break them down. Slowing down and chewing thoroughly reduces both drivers.
Eating in a calm, seated state activates the parasympathetic nervous system (your “rest and digest” state) and supports better gastric emptying.
Here’s what I recommend:
- choose a quiet space and sit at a proper table, without a cell phone or computer; avoid eating at your desk or behind your steering wheel!
- take 3 big inhales, and exhales to allow yourself to “land” in the moment
- setting a timer for 20 minutes to really take your time with your meal
- chew food thoroughly until applesauce texture
- set your fork down between bites
- notice the flavors and textures of foods, be curious what you note
- conclude with 3 more inhales and exhales at the end
- save beverages for between meals (not with)
- bonus: go for a short walk after
This is one of the simplest and most underestimated interventions for perimenopause GERD.
Adjust meal timing and size
Large meals dramatically increase pressure on the LES. Eating within two to three hours of lying down significantly worsens nighttime perimenopause GERD. Try smaller, more frequent meals and avoid eating within 3 hours before bedtime are among the most effective non-medication interventions.
Address sleep position
Elevating the head of your bed by 6-8 inches — using bed risers, not extra pillows — uses gravity to keep acid down during sleep. Left-side sleeping reduces reflux compared to right-side sleeping due to the anatomy of the stomach. Both changes make a meaningful difference.
Support the microbiome and gut lining
A healthy gut microbiome reduces bloating, supports gut motility, and decreases the intra-abdominal pressure that drives reflux symptoms. Emerging research is also exploring a fascinating connection between colonic bacterial fermentation and GERD — suggesting that changes in gastric and esophageal function may be driven not just by what’s happening in the stomach, but by increased bacterial fermentation further down in the colon (40).
This adds another layer to why gut microbiome health matters so much for women dealing with reflux in perimenopause. Supporting microbiome diversity through prebiotic foods, fermented foods, and targeted microbiome supporting protocols makes a foundational difference.
Read about prebiotic foods and gut health here. For fermented food options, this post walks you through how to ferment foods on your own at home.
Supporting the gut lining through zinc carnosine, L-glutamine, and anti-inflammatory dietary patterns reduces esophageal sensitivity to acid. Read more about 6 signs you might have leaky gut here.
Address Micronutrient Deficiencies
As discussed earlier, micronutrients play a dual role in the GERD picture for perimenopausal women. Some are depleted by the very medications used to treat reflux, while others are essential for healing the esophageal lining and protecting bone density.
Long-term PPI use depletes magnesium, calcium, B12, iron, and zinc — nutrients that are already under pressure from declining estrogen. That depletion compounds fracture risk at exactly the stage of life when bone loss is accelerating.
Specific nutrients like zinc carnosine, L-glutamine, and vitamin D directly support esophageal and gut lining repair. Because standard blood panels frequently miss tissue-level depletions, comprehensive micronutrient testing gives a far more accurate and individualized picture of what’s actually driving symptoms — and what needs to be repleted — for each woman.
Identify and remove food triggers
Conventional GERD management typically recommends avoiding common trigger foods — coffee, alcohol, chocolate, fatty foods, citrus, tomatoes, and mint. Removing these can bring some relief, but rarely fixes their symptoms. That’s because it addresses what irritates the esophagus without addressing what’s driving the inflammation underneath.
The research points to something more individualized. Research shows that women with GERD who weren’t responding to PPIs saw a 50% reduction in symptoms after just one month of removing their food sensitivities (29).
What this tells us is that the specific foods driving inflammation are different for every woman. A blanket elimination of common triggers misses the reactive foods that are actually fueling the problem for each individual.
In perimenopause, this matters even more. As the gut lining becomes more permeable due to estrogen decline, the immune system becomes increasingly reactive to foods it previously tolerated without issue (41). These immune-mediated reactions drive chronic gut inflammation that worsens bloating, motility issues, and reflux symptoms. This can happen often without any obvious connection to a specific meal or food group (42).
Food sensitivity testing that identifies each woman’s specific reactive foods is what actually moves the needle. It’s not about eating less of everything — it’s about knowing exactly what your immune system is reacting to and building a diet around that information.
A Perimenopause GERD Case Study
A client came to me in her mid 40s with GERD so painful it was waking her up before she’d even had breakfast. Her doctor prescribed her pain medication because her stomach pain was so intense. The pain medication made her sleepy so by 2pm she was hitting a wall so hard she needed a nap just to function.
She’d been on a PPI for six months before we met — if you’re not familiar with why that’s a problem, PPIs are only designed for short term use of around two weeks. Read more here. On top of that she had cycle related migraines nobody had connected to anything, weight gain through her midsection, and fatigue that made no sense given she was sleeping eight hours a night.
We ran food sensitivity testing, microbiome testing, and a micronutrient panel. What came back finally made sense of everything she’d been experiencing.
Phase 1: Food Sensitivities and Diet
Her food sensitivity results showed reactivity to corn, soy lecithin, and tyramine. The tyramine result was a significant moment — tyramine is a well documented migraine trigger and her doctors had never connected that.
Just by removing her reactive foods:
- In the first two weeks, stomach pain and refulx was significantly subsiding
- She started to notice she wasn’t needing her pain medication as often
- By week 6 she’d weaned off it entirely (with her doctor’s guidance)
- Her 2pm energy crash disappeared
- She wasn’t having migraines anymore!
- She became confident in knowing exactly which foods were working for her (and which ones were working against her)
- She became a wiz at reading food labels and cooking simple meals at home
Phase 2: Microbiome Rebalancing
Her microbiome results showed high LPS producing bacteria and significant fermentation in her colon. Research suggests colonic fermentation can drive upper GI symptoms including reflux through the pressure it creates from below (40). Because dietary inflammation had already been cleared in phase one, she felt this layer of work immediately. We were going another layer deeper now to address the root causes of where her digestive inflammation was stemming from.
Phase 3: Micronutrients
Her micronutrient panel showed low magnesium, vitamin A, vitamin C, zinc, vitamin D, and amino acids. Six months on a PPI had been quietly depleting her nutrient levels the entire time — PPIs impair absorption of micronutrients through reduced stomach acid (43). Her deficiencies were a direct consequence of the medication meant to “help” her.
Here’s what we addressed and why:
- Magnesium for gentle hormonal support and gut motility
- Vitamin A to support luteal phase progesterone productin + help heal the esophageal tissue
- Vitamin C which naturally supports luteal phase progesterone production and stomach lining repair
- Zinc carnosine to heal the stomach lining and intestinal permeability driving her food sensitivities.
- Vitamin D which supports immune function in the gut and has progesterone-like activity in the body (44)
- Gentle herbal support for her hormone fluctuation symptoms including poor sleep and achy joints — an area of expertise that made a meaningful difference alongside everything else
We also optimized her diet for microbiome health with polyphenol rich foods, diverse fiber, and prebiotic foods.
Three Months Later
She started riding her bike again. The stomach pain that had been so intense she couldn’t exercise was completely gone. She joined a group riding community she hadn’t been able to participate with in months. She felt confident knowing her food triggers, could navigate eating out confidently, and had the energy to show up fully at work and still care for her aging parents.
Her GERD was never about too much stomach acid or eating acidic foods. It was a layered picture — hormones, food sensitivities, microbiome imbalances, and nutrient depletions all contributing at once. When we addressed all of it together, her body responded incredibly.
When to See Your Doctor About Perimenopause GERD
Most perimenopause GERD responds well to the root-cause approach described above. If reflux is part of your perimenopause picture, a GERD dietitian nutritionist can help you find what’s actually triggering it.
Some situations need urgent medical evaluation. See your doctor promptly if you experience:
- Difficulty swallowing or a sensation that food is getting stuck in your throat
- Unintentional weight loss alongside perimenopause GERD symptoms
- Vomiting blood or black tarry stools
- Symptoms that don’t respond to any dietary or lifestyle changes after several weeks
- Chest pain — always rule out cardiac causes first
Your Next Step With Perimenopause GERD
Perimenopause GERD is a layered problem. Hormonal changes, gut motility, microbiome disruption, food sensitivities, structural factors, and lifestyle all contribute simultaneously. Addressing one layer without the others explains why so many women find temporary relief but not lasting resolution.
- Download the free 5-Day Gut Healing Plan — five days of what I teach my clients from day one, including strategies that directly support perimenopause GERD
- Book a free Digestive Assessment Call — a conversation about your specific perimenopause GERD situation and what’s driving your symptoms
- Learn more about working with a Perimenopause Gut Health Dietitian — 3-months of personalized coaching for women who want root-cause answers for perimenopause GERD and beyond
- If you’re struggling with IBS symptoms on top of GERD, my Midlife IBS Quiz takes 3 minutes to assess whether hormones are playing a role.

With over 20 years of experience, Sarah Neumann Haske, MS, RDN, specializes in helping clients resolve chronic digestive issues through a root-cause approach. She holds a Master of Science in Human Nutrition, is a Certified Microbiome Analyst, and is the owner of Neumann Nutrition & Wellness, LLC. Through her 3-month gut healing program, clients can reduce reliance on medications, improve energy levels, and achieve sustainable, long-term healing.
- Sarah Haske, MS, RDN

- Sarah Haske, MS, RDN
- Sarah Haske, MS, RDN
- Sarah Haske, MS, RDN