I’m Sarah Neumann Haske, MS, RDN — a gut health dietitian with over 20 years of clinical experience, specializing in perimenopause and digestive health for the past 10 years. If you’ve spent any time on TikTok or Instagram lately you’ve probably seen the viral trend of women taking antihistamines for perimenopause symptoms by combining Allegra or Zyrtec with Pepcid to manage hot flashes, brain fog, anxiety, and mood swings.
The global antihistamine market is valued at over $30 billion. Before you add to that number, here’s what the research actually shows about taking antihistamines for perimenopause symptoms daily.
The trend for taking antihistamines to calm perimenopause symptoms has gone massively viral and I’ve been getting questions about it from clients. In this post I’ll walk you through what’s actually going on when women take antihistamines for perimenopause, why the antihistamine trend misses the mark, and what actually gets to the root of healing perimenopause symptoms.
Histamine is just one piece of a bigger gut and hormone picture —you can learn more about what it’s like to work with a Perimenopause Gut Health Dietitian.
Want to start understanding your gut symptoms better right now?
- Download the free 5-Day Gut Healing Plan — five days of what I teach my clients from day one.
- Or book a free Digestive Assessment Call to see if my 3 month gut coaching program is the right fit for you.
- If you’re struggling with IBS symptoms alongside histamine symptoms, my Midlife IBS Quiz takes 3 minutes to assess whether hormones are playing a role.
Antihistamines for Perimenopause: How Your Hormones Drive Histamine
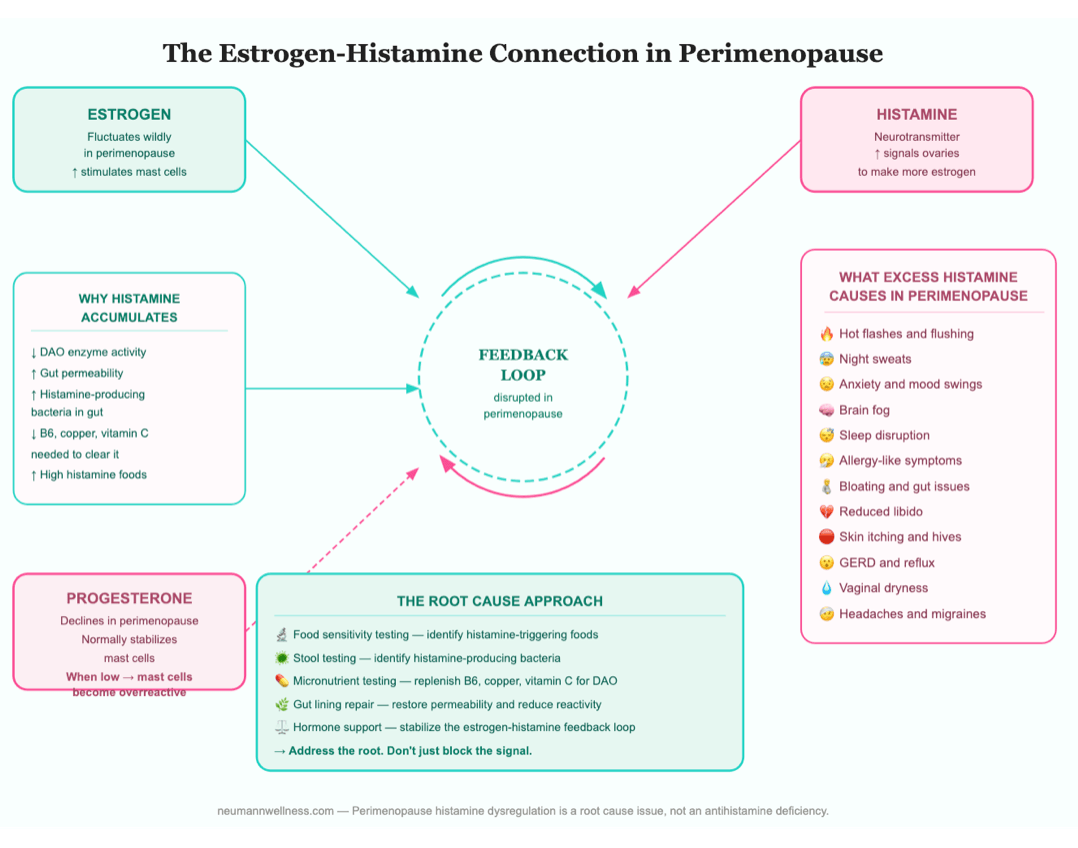
Most people think of histamine as just an allergy chemical. But histamine can also act as a neurotransmitter — a brain signaling molecule that plays a critical role in wakefulness, mood, cognition, memory, and hormonal regulation (1). It’s produced throughout the body but it’s particularly concentrated in the gut, skin, and lungs.
The Estrogen and Histamine Feedback Loop
Estrogen and histamine have a relationship most healthcare providers don’t know about. It typically peaks between days 7 and 14 of your cycle during your follicular phase. Estrogen produced in your follicular phase can activate immune cells called mast cells, which are immune cells that store and release histamine (2).
In perimenopause, when estrogen is fluctuating wildly from low to high. Cycles with higher amounts of estrogen cause histamine release to be amplified.
That histamine then signals the ovaries to produce more estrogen, keeping you stuck in a loop (3).
On top of that, if you’re dealing with new onset food sensitivities or environmental allergens, your estrogen can make mast cells even more trigger-happy — meaning less is needed to set off histamine production (2), (4).
Progesterone, the Histamine Brake
Progesterone on the other hand, can put a natural brake on the histamine loop as it typically increases after ovulation in the luteal phase of your cycle (5).
But in perimenopause cycles are frequently anovulatory (meaning ovulation doesn’t happen) so progesterone never rises to pump the brakes on histamine production.
The result is an increasingly reactive system producing more histamine than it did at baseline. That’s why so many perimenopausal women start noticing allergy-like symptoms, flushing, itching, anxiety, and sleep disruption they never had before.
What This Means for Your Cycle and Your Symptoms
It’s worth noting that f you have endometriosis it can amplify histamine production even further as endometriotic lesions recruit and activate mast cells locally (6).
On top of that, xenoestrogens (a synthetic estrogen-mimicking chemical found in BPA and phthalates) act as external drivers of mast cell activation even when your own estrogen production isn’t peaking (7).
Taking a daily H1 antihistamine like Zyrtec can interfere with your ability to ovulate (and produce histamine blocking progesterone) each month as histamine plays a direct role in stimulating the release of Luteinizing Hormone (LH), which is responsible for prompting ovulation to occur.
Blocking histamine with an H1 antihistamine disrupts that signal, potentially affecting ovulation and therefore reducing progesterone production (8).
Putting the Hormone Pieces Together
Antihistamines for perimenopause makes sense on the surface but as you can see, once you dig deeper to understand how taking a daily anti-histamine is actually breaking down important natural bodily processes. It’s worth taking a pause to consider greater health implications.
Every symptom your body is producing is a signal. Blocking that signal with a daily antihistamine doesn’t resolve what’s driving it — it just turns down the volume while the problem keeps running underneath.
Additional Reasons Why Antihistamines for Perimenopause Aren’t the Answer
Before you try antihistamines for perimenopause symptoms, here’s what nobody in the TikTok comments is mentioning:
- Blocking histamine affects your brain. Histamine is a neurotransmitter that plays a critical role in wakefulness, mood, cognition, memory, and hormonal regulation (1). When you block it you’re not just quieting an immune reaction, you’re interfering with brain signaling that affects how alert, focused, and emotionally regulated you feel. For women already dealing with brain fog and mood changes in perimenopause, that’s worth thinking carefully about.
- Taking antihistamines can dry out your vaginal tissue. Antihistamines dry out mucus membranes throughout your entire body, including vaginal tissue. In perimenopause when vaginal dryness is already a common and distressing symptom, adding an antihistamine makes it significantly worse (9).
- Antihistamines reduce your sex drive. Histamine plays a direct role in sexual arousal and desire. Blocking it reduces libido and can make arousal more difficult at a stage of life when it’s already taking a hit from declining hormones (10).
- Regular antihistamine use reduces stomach acid production. H2 antihistamines like Pepcid block histamine receptors on the cells that produce stomach acid. Low stomach acid impairs protein digestion, nutrient absorption, and your gut’s natural protection against infection, which is already a concern for many perimenopausal women (11).
- There’s no clinical evidence antihistamines for for perimenopause symptoms works. The trend is based on anecdotal reports and social media buzz, not clinical trials. No regulatory body has approved antihistamines for perimenopause symptom management.
If any of this gives you pause, that’s exactly the point. To understand why antihistamines for perimenopause carry these risks, it helps to know that not all antihistamines work in the same way.
Understanding the 2 Types of Anti-histamines
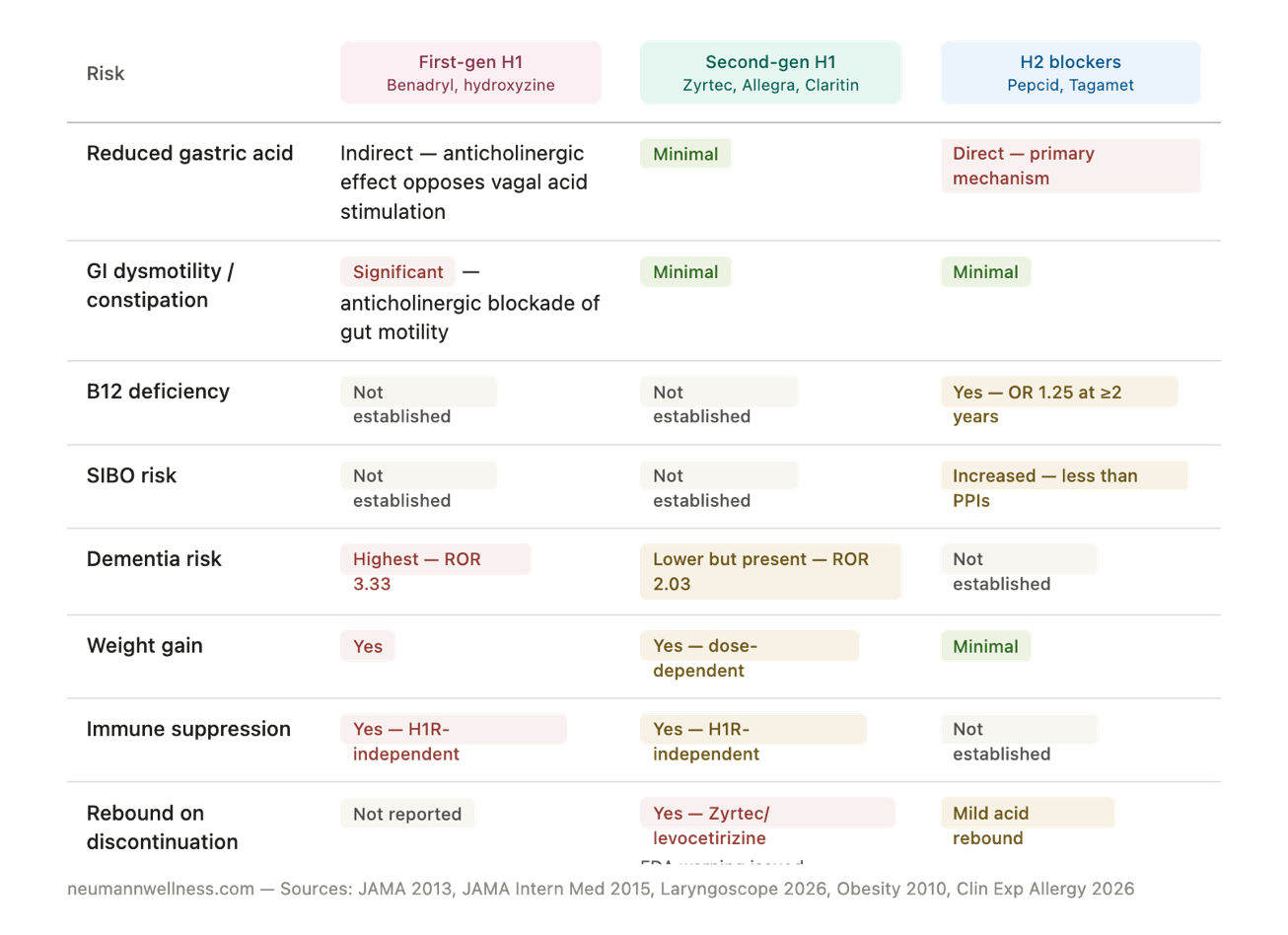
It helps to understand that not all antihistamines are the same. There are two completely different classes and most people taking the viral perimenopause protocol have no idea they work differently or carry different risks.
H1 antihistamines are the allergy medications — Benadryl (diphenhydramine), Zyrtec (cetirizine), Allegra (fexofenadine), and Claritin (loratadine). These block H1 receptors found throughout the body in the skin, lungs, and brain.
H2 antihistamines are acid suppressants — Pepcid (famotidine) and Tagamet (cimetidine). These block H2 receptors that sit directly on the acid-producing cells in your stomach.
The reason this distinction matters is that stomach cells express H2 receptors but not H1 receptors. This means H1 antihistamines like Zyrtec and Allegra don’t directly affect stomach acid at all.
That part of the viral protocol is entirely coming from the Pepcid — a dedicated acid-suppressing drug — whether it’s being taken for allergies, heartburn, or perimenopause symptoms.
The Risks of H2 Antihistamines (Pepcid, Tagamet)
As stated above, H2 antihistamines work by blocking the H2 receptors that sit directly on the acid-producing cells in your stomach. Taking H2 antihistamines for perimenopause symptoms comes with consequences most women aren’t warned about.
- They stop working almost immediately. H2 blockers lose 13 to 27% of their efficacy by day 15, a phenomenon called tachyphylaxis (when your body adapts to a drug and it becomes progressively less effective) (12).
- When you stop, acid comes back stronger. Chronic use causes your stomach to ramp up acid-producing capacity, so when you stop, acid rebounds worse than before you started (13).
- They deplete key nutrients your body needs. H2 blockers reduce stomach acid, which is essential for absorbing vitamin B12 (14), iron (15), calcium (16), folate (17), zinc, and magnesium (18). For perimenopausal women already navigating fatigue, brain fog, bone loss, and hormonal shifts, depleting all of these simultaneously is not a small thing.
- They increase your risk of gut infections and bacterial overgrowth. Stomach acid is your first line of defense against bacteria. H2 blockers reduce that barrier, increasing the risk of SIBO (small intestinal bacterial overgrowth) and serious infections including C. difficile, pneumonia, and peritonitis. (19), (20), (21).
If you’re taking Pepcid daily hoping it will help your perimenopause symptoms, the research suggests it will stop helping quickly while creating a new set of problems over the long term.
The Risks of H1 Antihistamines (Benadryl, Zyrtec, Allegra, Claritin)
H1 antihistamines come in two generations and their risk profiles are meaningfully different. Here’s what you need to know about each before taking antihistamines for perimenopause symptoms daily.
Pepcid stops working within two weeks, depletes the nutrients your bones and brain depend on, and makes your acid problem worse when you stop. That’s a lot of collateral damage for a trend that was never clinically tested for perimenopause symptoms.
First Generation H1 Antihistamines (Benadryl, Hydroxyzine)
First generation antihistamines like Benadryl have strong anticholinergic effects, meaning they block a key part of your nervous system that controls digestion, heart rate, and bladder function. In the gut this means dry mouth, constipation, and significantly slowed motility (22).
They also directly oppose the Vagal Nerve Stimulation (VNS) that triggers normal stomach acid production, compounding low stomach acid in susceptible women (23).
Here’s why VNS matters. Digestion doesn’t start when food hits your stomach. It starts the moment you see or smell food. Your vagus nerve sends a signal to your stomach to start producing acid before you even take a bite. First generation antihistamines block those same nerve signals, essentially telling your stomach to stop making stomach acid that breaks down foods (24).
The VNS also controls how quickly your stomach empties and the amount of digestive enzymes your pancreas releases. First generation antihistamines can disrupt your entire digestive process making it difficult to properly digest and breakdown foods leading to symptoms of fullness, gas, bloating, and constipation (24).
Another concern for midlife women is the brain. A landmark study of over 3,400 people followed for 7 years found cumulative anticholinergic use was associated with significantly increased dementia risk, with over 70% of cases diagnosed as Alzheimer’s disease (25).
First generation antihistamines are on the American Geriatrics Society’s explicit list of drugs older adults should avoid. Taking them daily for perimenopause symptoms while already navigating brain fog, mood changes, and cognitive shifts is a risk worth taking seriously.
Second Generation H1 Antihistamines (Zyrtec, Allegra, Claritin)
Second generation antihistamines may not significantly affect gut motility or acid secretion, but they carry their own risks. It’s worth noting First Generation H1 Antihistamines also carry the following risks too:
- Weight gain, higher waist circumference, and insulin resistance are all associated with regular use. NHANES data confirmed prescription H1 antihistamine users had significantly higher weight and insulin concentrations than matched controls (26).
- The immune system gets compromised through a pathway completely independent of histamine. This means more frequent infections, longer recovery times, and reduced ability to fight off the bacteria, viruses, and cancer cells (27), (28).
- Efficacy drops off within 7 to 21 days through receptor subsensitivity that cannot be overcome by doubling the dose (29) (30).
The Zyrtec Dependency Problem Nobody Talks About
The FDA has issued a specific safety warning about Zyrtec (cetirizine) and levocetirizine regarding rebound itching and hives when you stop taking them. A 2026 scoping review found symptoms develop within 1 to 5 days of stopping, affect women 76% of the time, and tapering only resolved symptoms in 33% of cases (31).
Many women find themselves unable to stop without their skin going haywire, not because their histamine problem has been addressed, but because their body has become dependent on the drug. This is one more reason why taking antihistamines for perimenopause symptoms daily creates more problems than it solves.
The FDA has warned that Zyrtec creates dependency. 76% of people who experience rebound symptoms when stopping are women. Tapering only works 33% of the time. This is not a supplement. This is a daily drug with a documented withdrawal pattern.
Before You Take Antihistamines for Perimenopause Daily, Ask Yourself This
The global antihistamine market is valued at over $30 billion and growing. When a medication generates that kind of revenue, long term safety research tends to take a back seat to marketing. The research links I’ve presented here are the bare minimum of what we actually know. Few studies look at long term implications beyond just a few weeks.
Antihistamines are over-the-counter (OTC) drugs that require no prescription, no doctor visit, and no oversight. It’s worth pausing to ask who benefits most from a viral TikTok trend that has millions of perimenopausal women reaching for a daily pill?
When Histamine Sensitivity Goes Deeper — MCAS, POTS, and Dysautonomia
Some women in perimenopause aren’t just dealing with elevated histamine from hormonal shifts. They have what practitioners in the functional medicine and integrative space are increasingly recognizing as Dysautonomia.
Dysautonomia is an umbrella term for conditions where the autonomic nervous system stops working properly. The autonomic nervous system is the part of your nervous system that automatically controls heart rate, blood pressure, digestion, and temperature regulation without you having to think about it.
Dysautonomia conditions like Mast Cell Activtation Syndrome (MCAS) and Postural Orthostatic Tachycardia Syndrome (POTS) can frequently co-occur with histamine issues.
Women with dysautonomia can have a nervous system and immune system that are chronically over-reactive, often rooted in deeper dysregulation that conventional medicine hasn’t connected the dots on.
Mast Cell Activation Syndrome (MCAS)
MCAS is one of the most significant conditions in this category. Mast cells are the immune cells that store and release histamine. In MCAS those cells activate inappropriately and release massive amounts of histamine and other inflammatory mediators in response to triggers that wouldn’t bother most people (31).
This extra histamine can be released in response to certain foods, smells, stress, temperature changes, even exercise. GI symptoms occur in 14 to 85% of people with MCAS and include heartburn, abdominal pain, diarrhea, and reflux (31).
Acute mast cell activation can cause hyperacidity through histamine’s direct effect on stomach acid-producing cells, while chronic mast cell-mediated inflammation can eventually damage those same cells and reduce acid production over time (32).
An antihistamine doesn’t fix a leaky gut, rebalance a dysbiotic microbiome, replenish depleted nutrients, or stabilize hormonal histamine signaling. It blocks a signal your body is sending for a reason.
POTS (Postural Orthostatic Tachycardia Syndrome)
POTS occurs when your heart rate spikes dramatically just from standing up and other forms of dysautonomia (your autonomic nervous system that controls heart rate, digestion, and blood pressure) — stops regulating properly) frequently co-occur with MCAS and histamine intolerance.
Many women in perimenopause who have spent years being dismissed with vague overlapping symptoms find that these conditions finally explain their picture.
If any of this resonates, know that the gut health and nutrition piece is always foundational — even for these more complex conditions. Histamine-producing bacteria, intestinal permeability, food sensitivities, and nutrient deficiencies that impair your body’s ability to break down and clear histamine are all gut-rooted drivers that sit underneath the bigger picture.
Consider the Bigger Picture
Addressing foundational layers through comprehensive stool testing, food sensitivity testing, and micronutrient testing creates a more stable internal environment that makes every other intervention work better.
These are exactly the layers I work through with clients who are dealing with histamine reactivity in perimenopause — and addressing them consistently moves the needle in ways that taking an antihistamine every day simply cannot.
High Histamine Foods Worth Knowing About
If you suspect histamine is playing a role in your perimenopause symptoms, your diet is a good place to start. High histamine foods include:
- Aged cheeses
- Red wine and alcohol
- Fermented foods like sauerkraut, kimchi, and kombucha
- Cured and processed meats
- Smoked fish
- Vinegar and vinegar-containing foods
- Leftovers (histamine increases the longer food sits)
- Canned and preserved foods
Removing high histamine foods can bring real relief for some women. But it often doesn’t fully resolve symptoms because histamine reactivity in perimenopause isn’t just about what you’re eating.
It’s about how your immune system is responding to what you’re eating.
What Actually Gets to the Root of High Histamine in Perimenopause
The reason histamine is elevated in perimenopause isn’t because you have an antihistamine deficiency. It’s because your hormones are shifting, your gut microbiome is changing, and your body’s ability to break down and clear histamine has been compromised (33), (34).
Your gut produces an enzyme called DAO (diamine oxidase) that breaks down histamine. When your gut lining becomes more permeable (which happens as estrogen declines) DAO activity drops and histamine accumulates (34).
Certain gut bacteria also produce histamine directly, and the microbiome shifts of perimenopause can increase those histamine-producing populations.
This is where my work comes in. Food sensitivity testing identifies whether specific high histamine or histamine-liberating foods are actually driving your immune reactions. Comprehensive stool testing identifies whether histamine-producing bacteria are contributing to the load. And micronutrient testing can identify whether you’re deficient in the nutrients your body needs to produce DAO and break histamine down properly — particularly vitamin B6, copper, and vitamin C.
Taking an antihistamine might quiet the symptoms temporarily. But addressing why histamine is elevated in the first place is what actually resolves it — and has the added benefit of improving your digestion, your gut lining, your energy, and your hormonal balance at the same time.
Your Next Step
Histamine dysregulation in perimenopause is a layered problem. Hormonal changes, gut microbiome disruption, intestinal permeability, nutrient depletions, and food sensitivities all contribute simultaneously. Addressing one layer without the others explains why so many women find temporary relief but not lasting resolution.
- Download the free 5-Day Gut Healing Plan — five days of what I teach my clients from day one, including strategies that directly support histamine balance in perimenopause
- Learn more about working with a Perimenopause Gut Health Dietitian — 3 months of personalized coaching for women who want root-cause answers
- Book a free Digestive Assessment Call — a free call to talk through your symptoms and find out if my 3-month perimenopause gut coaching program is the right fit for you
- If you’re struggling with IBS symptoms alongside histamine symptoms, my Midlife IBS Quiz takes 3 minutes to assess whether hormones are playing a role

With over 20 years of experience, Sarah Neumann Haske, MS, RDN, specializes in helping clients resolve chronic digestive issues through a root-cause approach. She holds a Master of Science in Human Nutrition, is a Certified Microbiome Analyst, and is the owner of Neumann Nutrition & Wellness, LLC. Through her 3-month gut healing program, clients can reduce reliance on medications, improve energy levels, and achieve sustainable, long-term healing.
- Sarah Haske, MS, RDN

- Sarah Haske, MS, RDN
- Sarah Haske, MS, RDN
- Sarah Haske, MS, RDN